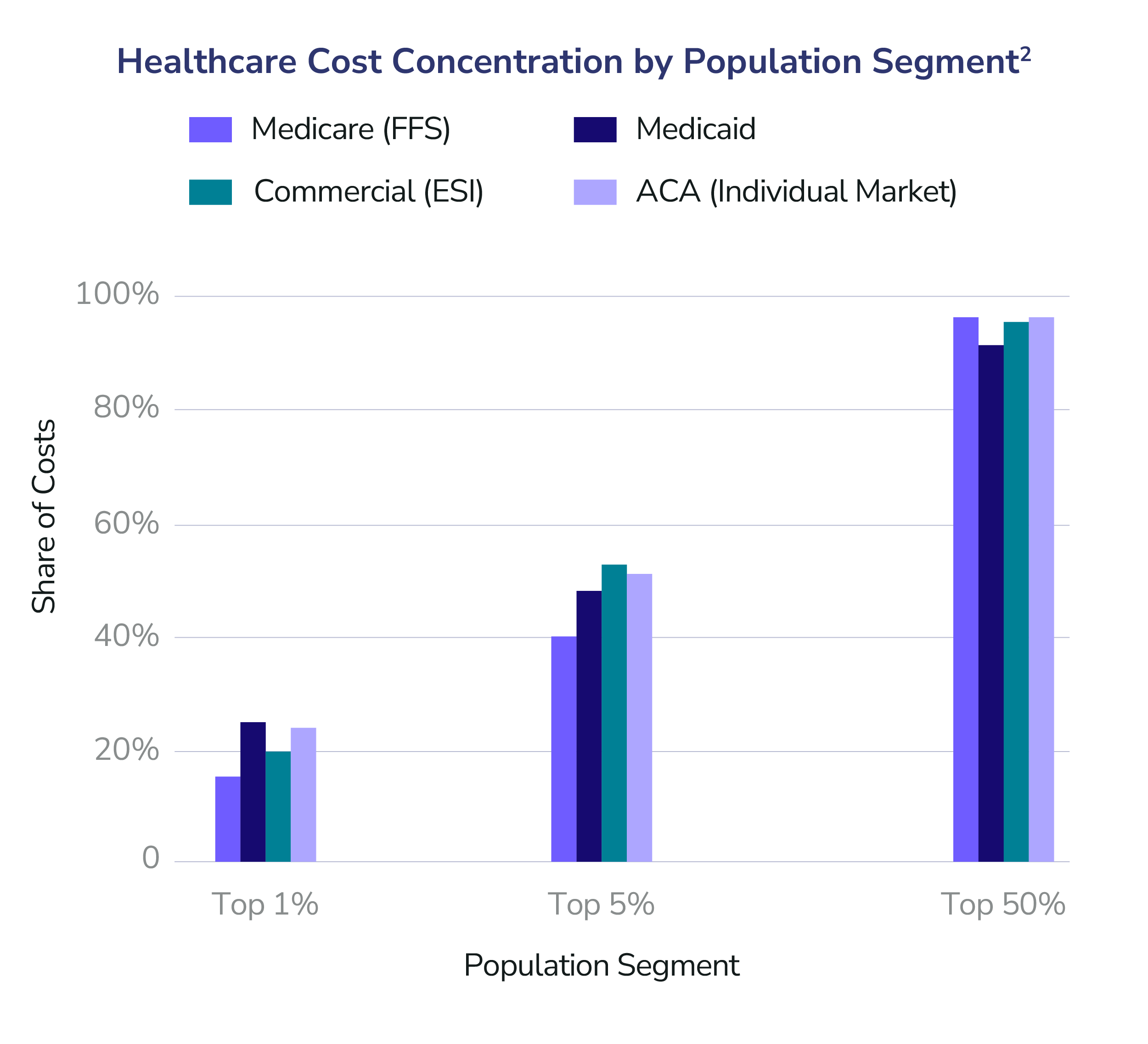
Healthcare spending is not evenly distributed. It never has been and the data is unequivocal. Across Medicare, Medicaid, commercial insurance, and ACA markets, a small fraction of patients account for the overwhelming majority of costs. Roughly 5% of patients consume 40–53% of total healthcare spending, while the healthiest 50% account for only 3–8%. In effect, healthcare expenses are incurred by a few and paid for by everyone.1
This imbalance and economic moral hazard — few consume while all pay — is not just an accounting curiosity, it is the central structural problem of modern healthcare. As long as payment models reward volume over outcomes and intervention over prevention, costs will continue to rise. Aging populations, higher chronic disease burden, and increasingly complex care needs will only accelerate this trend. Absent a fundamental shift in how care is financed and delivered, the math simply does not work and explodes as it continues.
What is often underappreciated, however, is how predictable high-cost care actually is. For nearly every patient with sufficient longitudinal claims and clinical data, there is a remarkably consistent pattern: escalating utilization, repeat admissions, medication changes, complications, and downstream events that follow known clinical pathways. These are not random surprises — they are foreseeable trajectories.
This is where precision AI and accountable care models change the equation. When providers are accountable for outcomes and supported by AI that can synthesize claims, clinical history, utilization patterns, and social risk, the next best actions become clear. Which patients are likely to deteriorate? Which admissions are preventable? Which interventions — clinical, behavioral, or social — will most likely bend the cost curve while improving quality of life? This process can in fact, once mastered, begin at the creation of life and is not just a clinical strategy for senior care.
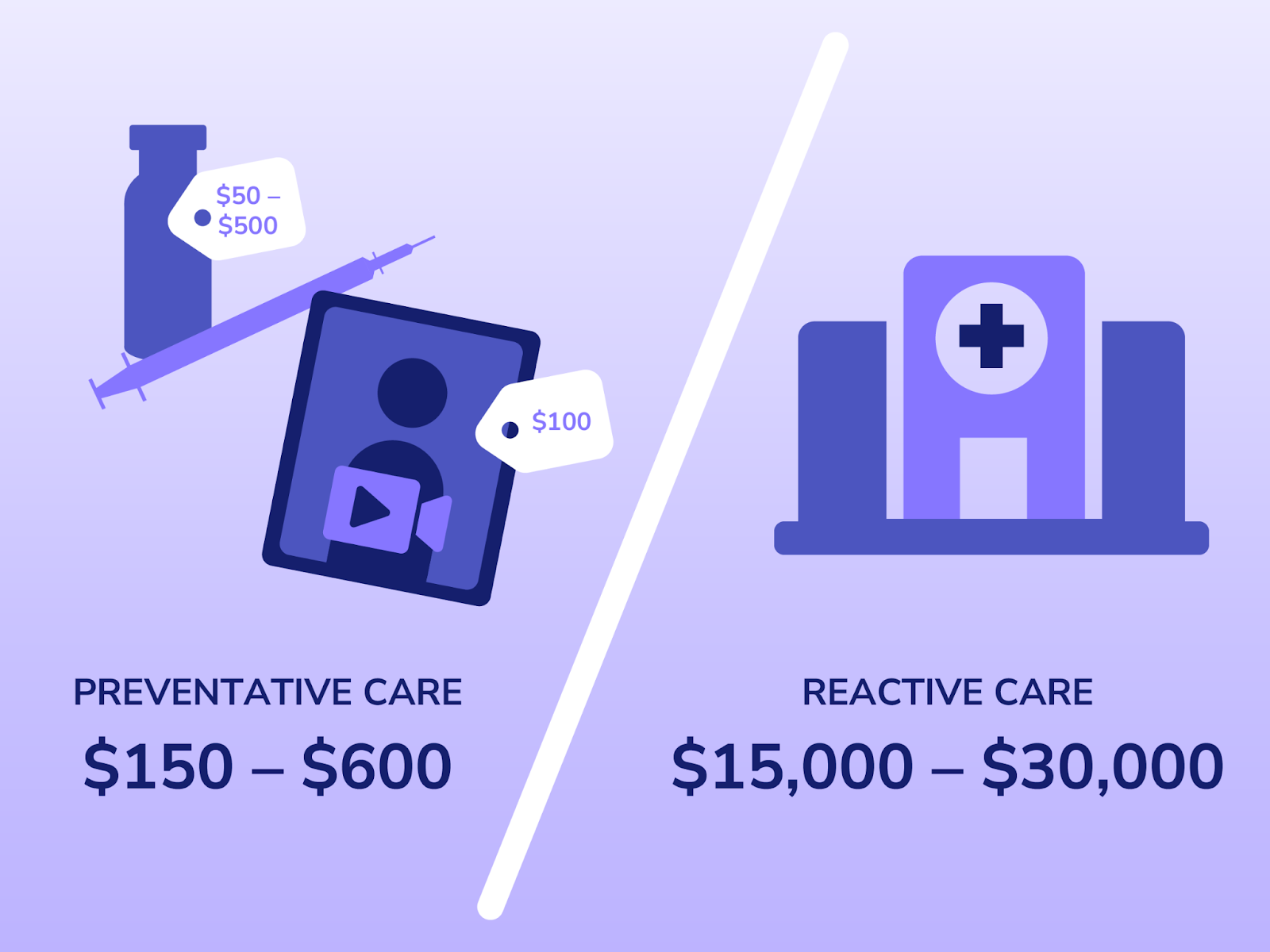
Crucially, delivering these interventions earlier should be dramatically cheaper than the costs we incur today. Preventing a hospitalization is less expensive than treating one. Coordinating care is cheaper than managing fragmentation. Supporting patients before crises emerge costs a fraction of reactive, late-stage care. Consider a simple, real-world example. A diabetic patient is struggling to reliably obtain insulin. The proactive intervention is straightforward: home delivery of insulin, costing roughly $50 – $500, combined with a digital physician consult of approximately $100. In total, the cost of stabilizing this patient in the moment is $150 – $600. The alternative, however, is all too familiar. A lapse in access leads to deterioration, an emergency department visit, and an avoidable hospitalization, with costs ranging from $15,000 to $30,000. The clinical pathway is predictable. The cost differential is stark. And yet, in a reactive system, we routinely pay for the latter instead of investing in the former.
The future of healthcare is not about managing averages. It is about precisely identifying the patients who drive cost, anticipating what they need next, and delivering that care proactively. If we are all going to continue to pay for each other's care we must reduce costs and disease through prevention and precision AI. With AI-enabled insight and accountable payment models aligned around outcomes, we can move from a reactive system that pays for failure to a proactive one that invests in health.
- National healthcare expenditure data from the Medical Expenditure Panel Survey (MEPS) shows that the top 5% of people account for nearly half of all healthcare spending, while the bottom 50% contribute only ~3% of total costs. At the extreme end, the top 1% alone accounts for over 20% of spending illustrating just how skewed healthcare utilization truly is.
- Medical Expenditure Panel Survey (MEPS).
Pearl Health is powering the future of healthcare
We’re a team of physicians, technologists, and risk-bearing experts with a passion for enabling our partners to deliver better care and reduce health system costs. Want to learn more?
