Lesson 1: Understand the origins of inefficient costs in healthcare.
Why is cost a problem, when in so many other industries market forces and buyer sensitivities would arrest this issue? There are three systemic drivers:
- Vulnerability: Healthcare needs strike at our greatest vulnerabilities, allowing for coercive forces that frustrate the normal dynamics of a competitive market. One generally cannot simply forgo a necessary healthcare service (though this is happening more and more in the US). Our vulnerability to our health is inherent to our existence, but can be mitigated by improving our health (or, in some cases, our knowledge).
- Locality: Local care delivery means fewer competitors that can offer services, allowing for less efficient and dynamic markets to flourish. The incremental adoption of digital and virtual healthcare can address aspects of this dynamic by making a competitive national marketplace for care delivery more practicable. But healthcare has faltered in transitioning to digital and virtual models. This has begun to change for those services where it is feasible (e.g. mental health services). Even where it is appropriate to deliver care in this modality, progress is slow due to the regulated nature of healthcare. For other services, it’s not feasible to move totally to a virtual model.
- The Triangle of Moral Hazard: patients want services, physicians bill for them, and insurers pay for them, all while almost no one knows what those services cost or the relative value of marginally more expensive services. This unawareness and indirect incentive structure creates waste. A good example of this phenomenon is the surf and turf conundrum, which can be summarized as the impression by patients that a ‘free rider’ phenomenon exists in healthcare (due to the intermediation of costs via health insurance), when in fact that is not true: we pay for increased utilization through higher insurance premiums, or degradation of the Medicare trust fund.
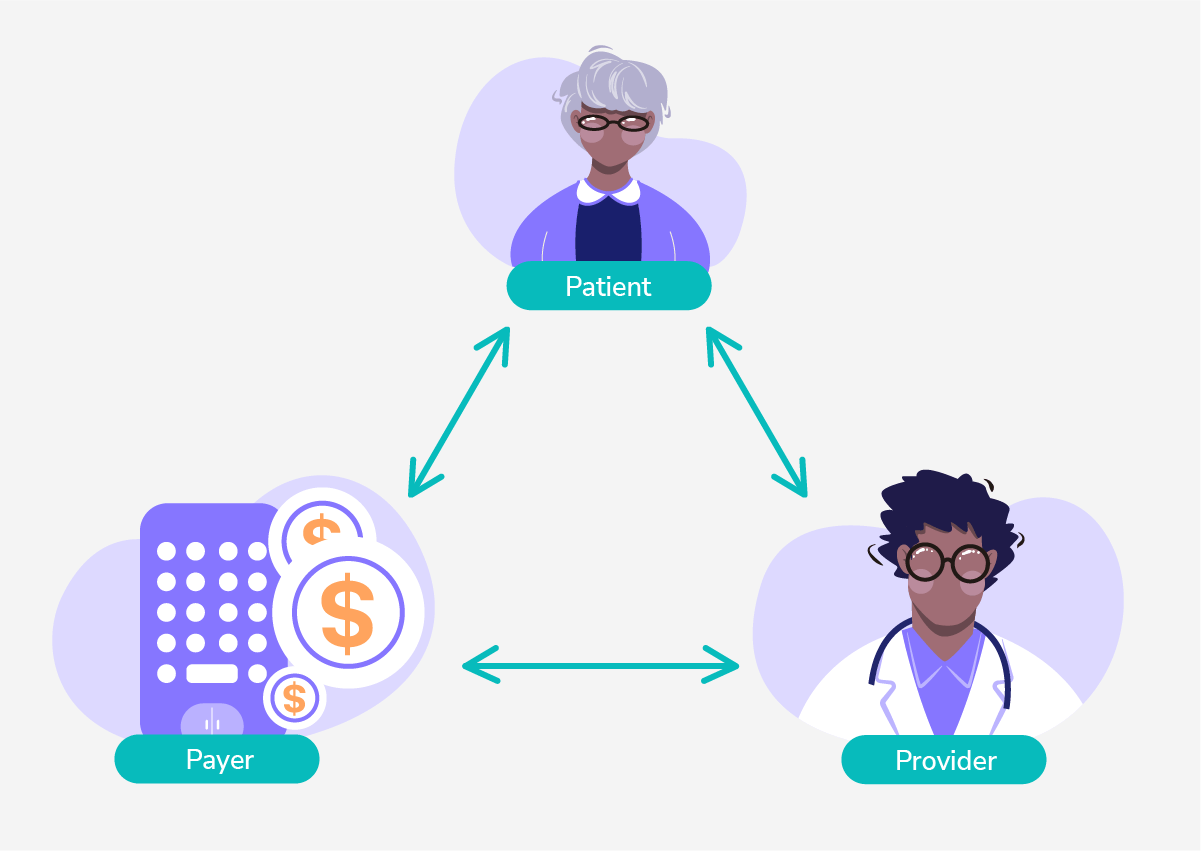
The Triangle may be addressed in two ways: transparency and incentives. By making costs more transparent to each actor and reorienting incentives (e.g. through micro-incentives, or nudges, for making responsible decisions), we can address persistent free-rider dynamics.
Lesson 2: Understand the causes of disease and disease progression.
We believe the root causes of disease can be bucketed into six origins1 :
- Genetics, or the inherited traits that may result in the generation of hereditary diseases or the increased propensity to develop a condition.
Appropriately conscientious utilization of this information can help identify future health problems and likely condition development, as well as provide guidance on the likely efficacy of certain medication classes.
- Previous Illness, or, simply, having been sick before.
Prior illnesses can be a powerful indicator of future health and guidance for health management efforts. While intaking a patient’s medical history is a standard of patient onboarding, the ability of technology to surface relevant information to providers at the moment of usefulness remains in its nascent stages. Improvements in data liquidity will help address this.
- Acute Events, or the impact of an adverse, unexpected event on one’s bodily function (e.g. a broken leg from an auto collision).
Acute events are the unpredictable everyday toll on health that results from living our lives. Good self care, timely prevention, and an efficiently connected healthcare system can help address the impact of these unavoidable events.
- Infections, or the contraction of a bacteria or virus, which may result in the development of an infectious disease or exacerbate other conditions.
Infections are a unique but important category within the bucket of acute events – they are a specific form of a largely unpredictable set of occurrences that may impact our health.
- Social Determinants of Health, or the background socioeconomic and physical conditions in which we live our lives, which have been proven to impact our health. The Department of Health and Human Services summarizes these forces through five domains:
- Economic Stability
- Education Access and Quality
- Healthcare Access and Quality
- Neighborhood and Built Environment
- Social and Community Context
While we do not undertake a thorough investigation of the ways in which we can address these societal forces, it suffices for the purpose of this article to acknowledge that, generally speaking, economic inequality breeds bad health outcomes.
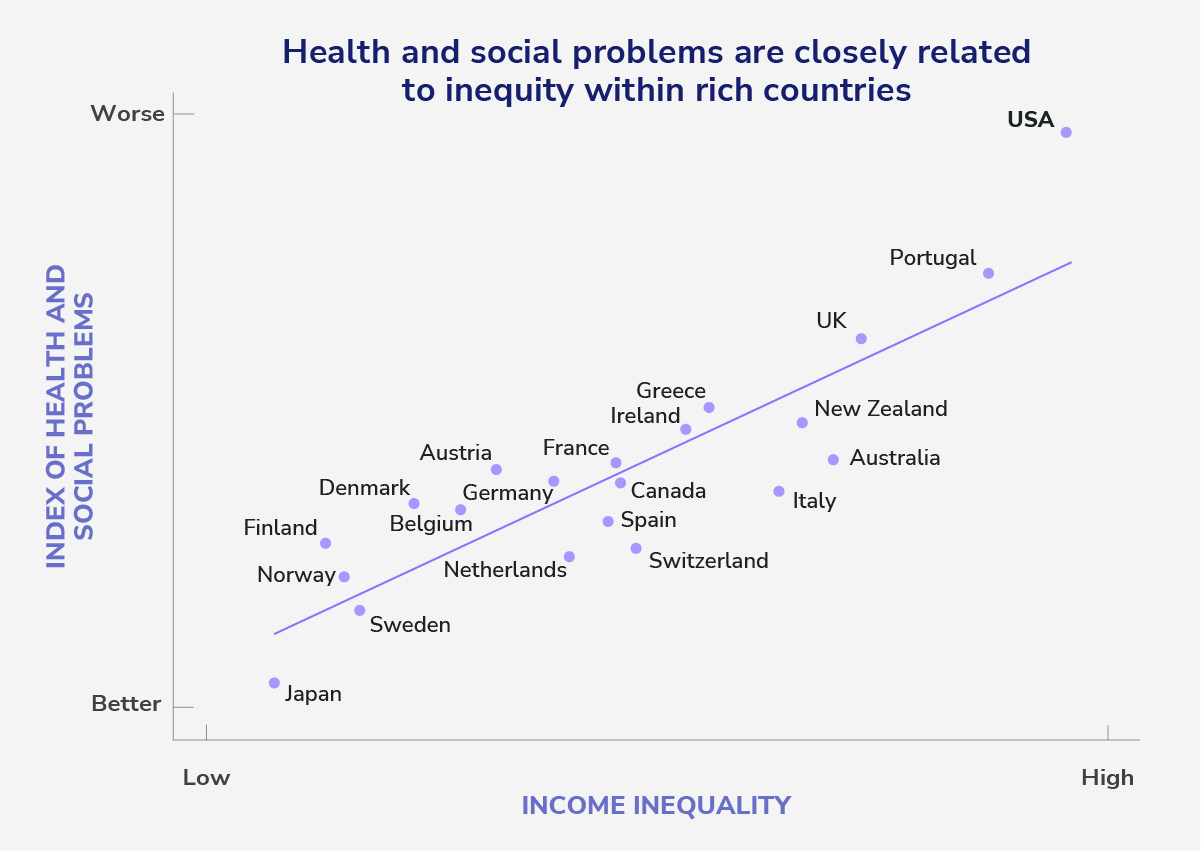
Source: Greater Equality: The Hidden Key to Better Health and Higher Scores
- Lifestyle, or the daily choices we all make that may impact our health, for better or worse, e.g. diet, exercise, etc.
Lifestyle, and the feedback loop it has to patient compliance with care protocols, is a critical component of patient health, and is inextricably connected with many of the other disease drivers outlined here. Yet it runs into the background forces precipitated by SDOH factors outlined above, hardwired habits and learned behaviors, while also running afoul of our innate human inability to appropriately price future risk versus present reward. While some have dug into the diligent protocols that can breed better compliance with care protocols, and we recognize the immeasurable value of such work, we also believe that appropriate incentives flip the cost-benefit analysis of everyday habits in a beneficial way. Financial incentives for healthy behavior will likely play a valuable role as more patients are managed in the context of at-risk provider programs.
Lesson 3: Focus on primary care.
Most of the above points can be boiled down into one key lesson: early identification and active management of conditions at lower-cost sites of service will reduce costs and improve outcomes. This truth points to the critical importance of primary care providers (PCPs) – those who are entrusted with managing the overall health of their patients before disease becomes acute enough to warrant more specialized or active intervention. They are best positioned to manage the longitudinal health of patients, but we need to do more to support them in these efforts. We can:
- Provide PCPs with economic structures that both incentivize and free them to engage their patients holistically and proactively.
At Pearl, we believe that the mixture of capitation (freedom to manage their patient panel in line with the needs of their patients, not maximizing volume) and total-cost-of-care risk exposure (financial incentives to engage them in managing that patient panel) is the key formula.
- Give PCPs the tools and insights they need to manage their patients effectively, empowering PCPs to identify patient needs and communicate with their patients in a low-friction and highly responsive manner.
Data should be easily accessible to those with the need for it and surfaced in an actionable way (i.e. at the moment it is most useful). One sample framework for thinking about how to prioritize panel management from a cost perspective is through a 3-axis categorization of care utilization: how frequently does the event happen in the patient population, how expensive is the event, and how likely is it that a PCP will be able to avert or otherwise mitigate the impact of the event.
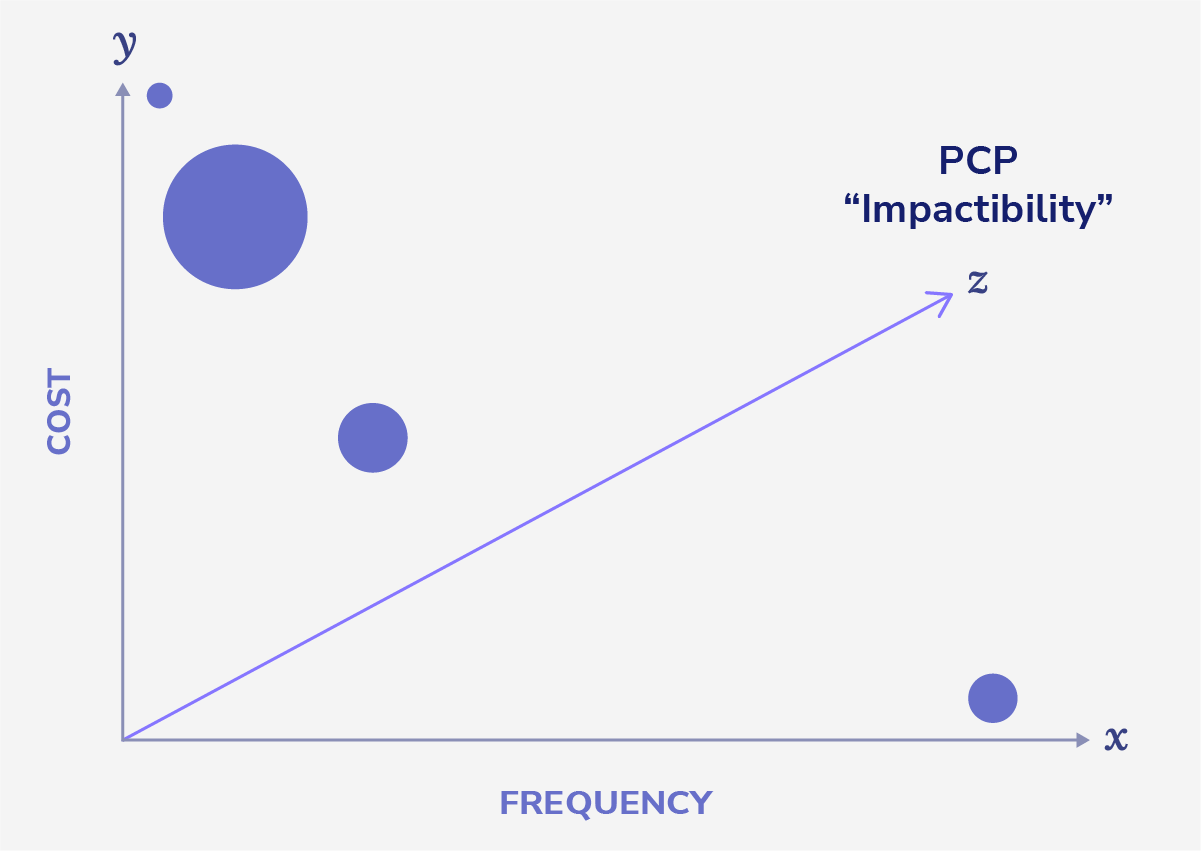
The above image demonstrates the framework, with the size of the points representing how far along the z-axis they are (i.e. larger bubbles are more likely to benefit from PCP intervention). Two illustrative examples:
- Urgent care utilization is likely moderate in frequency, relatively low-cost, but highly responsive to PCP engagement (e.g. through an after hours or ad hoc ability to communicate with a member of the care team);
- On the other end of the spectrum, expensive cancer treatment may be very high cost, but also infrequent and not at all impacted by PCP engagement.
Primary care enablement should focus on empowering PCPs to address utilization issues that strike the right balance, with a synthetic score likely informing the rank-order prioritization of those tasks.
- Mitigate the impact of low-value administrative tasks, either by (a) removing them, (b) automating them, or (c) empowering others to complete them.
When it comes to lifestyle and social determinants of health, it is also critical to empower PCPs with support services that they can engage their patients in, when specific risks or gaps in access are identified. For example, while it is not tenable for a PCP to plan out a diet plan for a pre-diabetic, allowing a PCP to flag that a given patient would benefit from such engagement, and delivering it automatically, would be hugely beneficial.
In Part II, we outlined the three conceptual lessons that anyone seeking to embark in value-based care should understand. In Part III, we will delineate tactics that will help providers set themselves up for success as they enter this new world.

